
Costochondritis…rib pain
I am writing this blog post today on the backdrop of the cold and flu season in the Southern Highlands. I’ve had more than one person tell me that it has been a particularly difficult Winter this year experiencing more than their fair share of virus’ which are doing the rounds. If you’ve ever been struck down by one of these bugs you’ll know that it can result in aches and pains from coughing, prolonged bed rest and awkward posturing from immobility. But how much of this is mechanical in nature and can a physiotherapist be of any help?
Today I thought I'd touch on Costochondritis which is inflammation of the costal cartilage in the chest wall. The costal cartilage is the point where our ribs attach to our sternum (front bone of the chest). Costochondritis can cause severe chest wall pain which can be point tender over the sternum or radiate out over the adjoining ribs. You’ll find that even breathing in and out, lifting heavy objects or any exertion can cause pain.
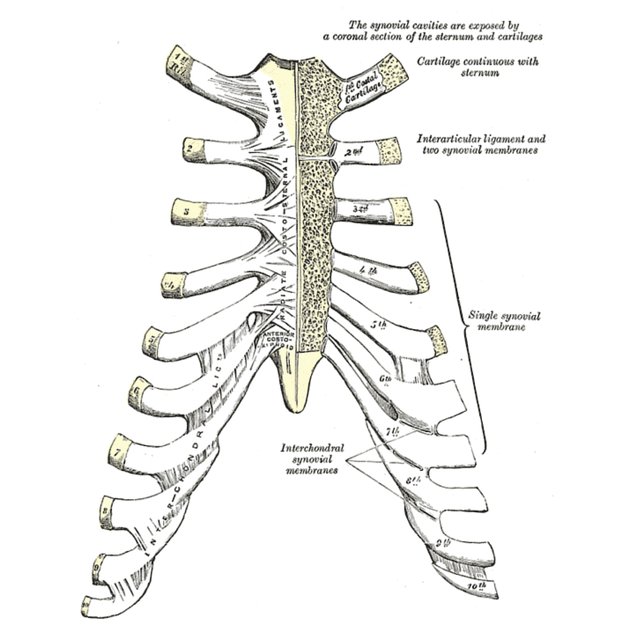
The ribcage - front (Radiopeadia)
Signs and symptoms include severe pain in the chest wall region and ribs, pain on palpation of the ribs, direct pressure particularly in bed or in prolonged sitting postures, pain on inspiration and expiration and shortness of breath (more so because it hurts to breathe). Costochondritis will occur more often due to a traumatic event such as a car accident or perhaps a tackle in rugby where there is direct impact to the region or in the case of illness, a severe cough.
Because this condition can be quite severe in terms of pain severity, some patients will say they feel they have fractured a rib (which can happen in some cases but more so with trauma or if the patient has bone density issues such as in the case of osteoporosis). In the early phases Costochondritis does not respond very well to manual therapy, if anything it can make it worse. Early phase therapy will include offloading strategies such as taping the shoulder girdle to enable better rib articulations, heat packs and plenty of them, NSAIDS/Paracetamol (as prescribed by your GP and pharmacist), assisted coughing such as placing a towel or pillow over the affected area when you cough, and mobility exercises such as gentle walking. Once patients move beyond those early phases we can begin regaining any joint mobility that has been lost and manual techniques for soft tissue.
Costochondritis is a benign self-limiting condition and will improve over time. This post is by no means to be used as a diagnostic tool. If you do have chest wall pain please present to your physician for assessment. You will require a compressive assessment to rule out other causes of chest wall pain including pneumonia and chronic lung disease (visceral referred pain from the lungs), Herpes zoster, fractures, post operative lung surgery, myocardial infarction (heart attack) and systemic disorders (to name a few).
As always Andrew and myself are here to answer any questions you may have about this or other posts.
Yours in health
Sam and Andy